



Menopause is not only a reproductive transition. It is also a neurological, metabolic, hormonal, and psychological transition that can affect mood, anxiety, sleep, cognition, libido, stress tolerance, and sense of self.
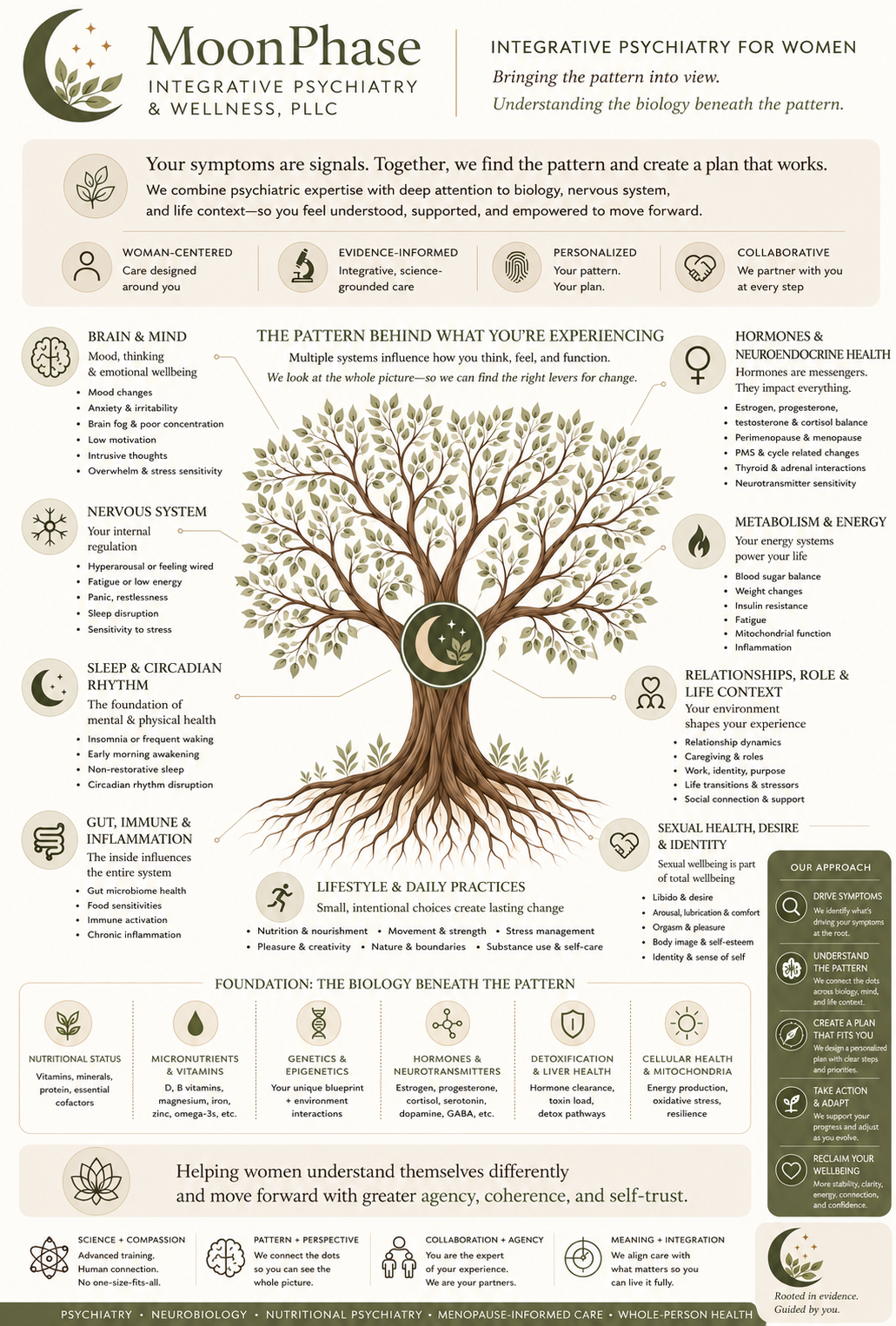
At MoonPhase Integrative Psychiatry & Wellness, menopause-informed mental health means looking beyond isolated symptoms to understand the larger biological, psychological, relational, and life-stage patterns shaping a woman’s experience.
We stay grounded in science while making space for thoughtful questions, personal values, and sustained support in women’s mental health care.
Why Menopause Belongs in Mental Health Care
A growing body of literature recognizes the menopausal transition as a clinically meaningful period for mood, anxiety, sleep, cognition, and psychiatric vulnerability.
At MoonPhase, this means integrating evidence-informed decision-making, current research, and clinical literature into thoughtful assessment, education, and individualized treatment planning.
Menopause Is a Mental Health Transition, Too
Menopause is increasingly recognized as a period of vulnerability for changes in mood, anxiety, sleep, cognition, and psychiatric symptom expression.
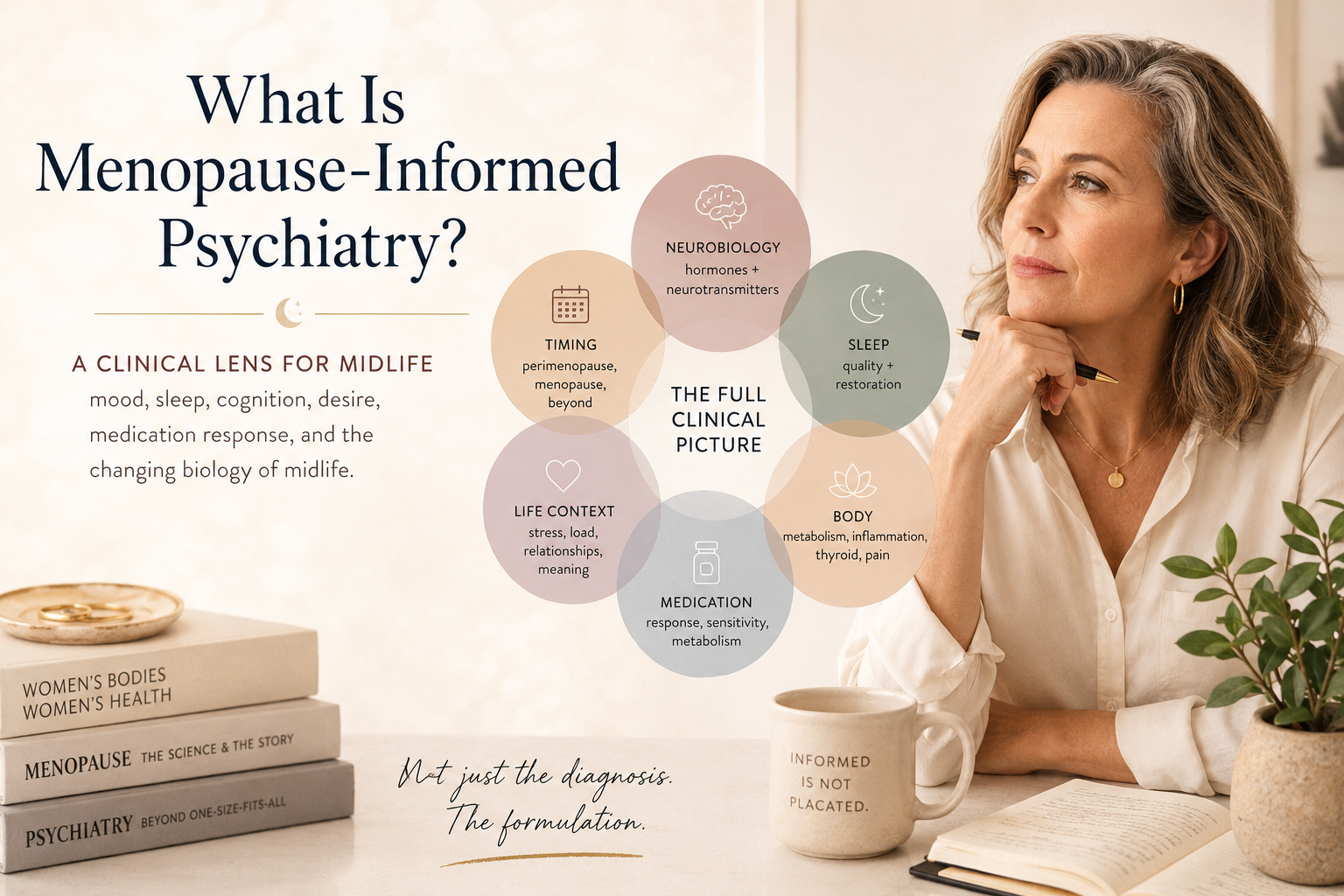
Menopause-informed mental health care does not reduce every symptom to hormones; rather, it considers hormonal transition as one important part of a broader psychiatric, medical, metabolic, relational, and life-stage context.
Midlife hormonal shifts can influence brain function, sleep architecture, neurotransmitter systems, inflammation, metabolism, and stress response.
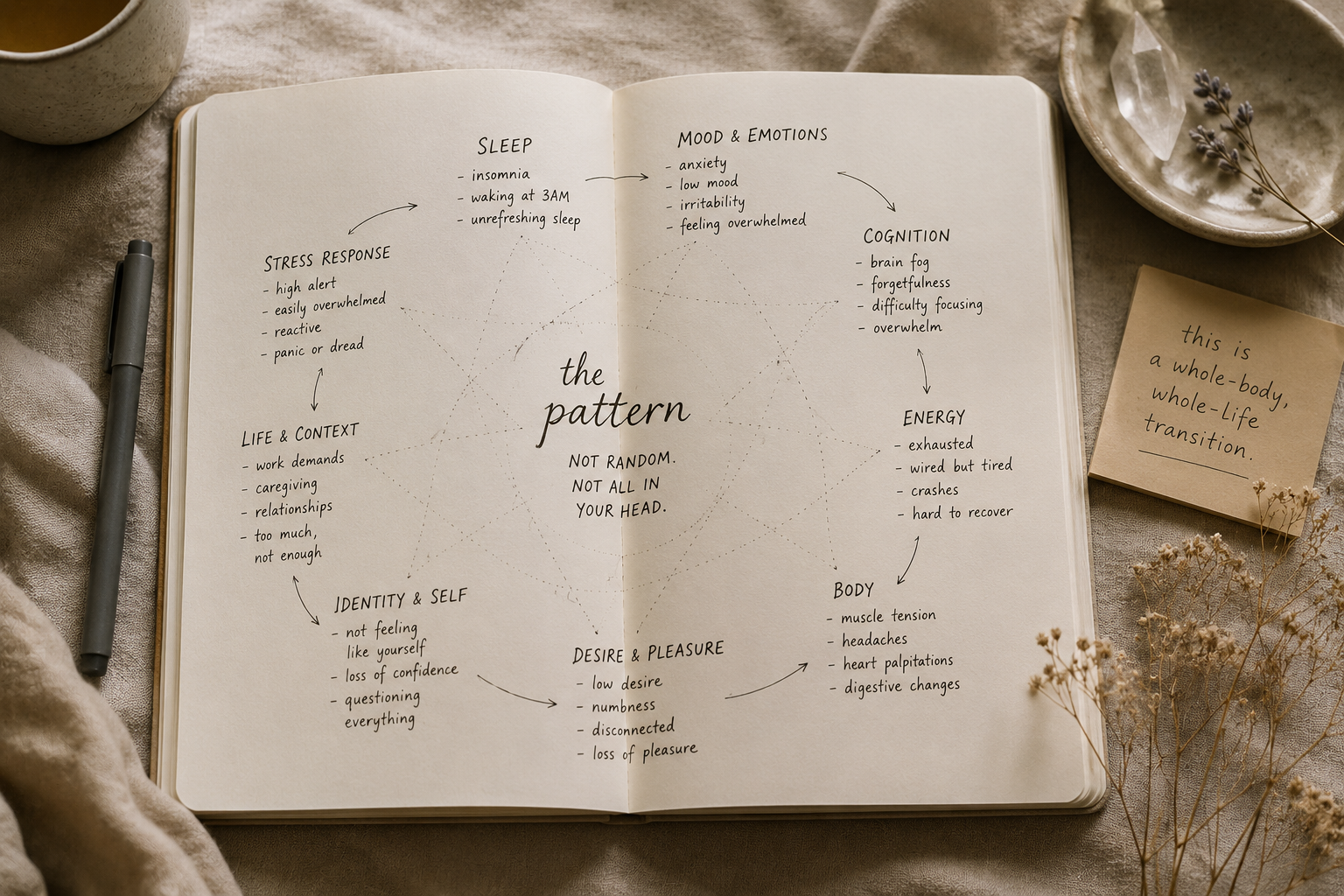
Why Symptoms Often Travel Together
Mood changes, anxiety, sleep disruption, brain fog, libido changes, irritability, and changes in desire often overlap because they may share underlying biological, psychological, relational, and lifestyle drivers.
At MoonPhase, these symptoms are not viewed in isolation. They are understood as part of a larger pattern that may involve hormone signaling, sleep disruption, stress physiology, medication effects, nutritional status, metabolic health, inflammation, identity shifts, and the demands of midlife.
The MoonPhase Lens
MoonPhase uses a care model that is:
Pattern-based
We look for connections across mood, anxiety, sleep, cognition, libido, stress tolerance, and sense of self.
Biology-rooted
We consider how hormonal transition, neurochemistry, metabolism, inflammation, nutrition, and medication response may shape symptoms.
Psychiatric
Assessment and treatment remain grounded in psychiatric evaluation, diagnostic clarity, medication strategy when appropriate, and therapeutic support.
Integrative
Care may include lifestyle medicine, nutritional psychiatry, supplement review, somatic practices, and lab or genetic testing when clinically appropriate.
Collaborative
When needed, MoonPhase may coordinate with primary care, gynecology, therapy, or specialty providers.
What Menopause-Informed Care Does & Does Not Mean
Menopause-informed care does not mean every symptom is “just hormones.” It means hormonal transition is considered as one meaningful part of a broader psychiatric, medical, metabolic, relational, and life-stage context.
This approach allows care to remain clinically grounded while honoring the complexity of women’s lived experience.
How This Shapes Care
At MoonPhase, menopause-informed mental health care may include comprehensive psychiatric assessment, medication strategy when appropriate, therapy-informed support, lifestyle and nutritional psychiatry, supplement review, lab or genetic testing when clinically indicated, and collaboration with primary care, gynecology, or other providers.
Scientific References
Menopause, Mood, Sleep, Cognition & Mental Health
The following nine peer-reviewed articles and professional guidelines inform the MoonPhase approach to menopause-informed psychiatric care. They are offered as educational resources and are not a substitute for individualized medical or psychiatric evaluation.
(article link will open new page)
1. Guidelines for the evaluation and treatment of perimenopausal depression
🩺 Link: https://pubmed.ncbi.nlm.nih.gov/30182804/
Summary:
This expert guideline provides clinical recommendations for evaluating and treating depression during the menopause transition. It supports assessing menopausal stage, depressive symptoms, anxiety, sleep, vasomotor symptoms, psychosocial stressors, medical contributors, and treatment history. It also helps distinguish when antidepressants, psychotherapy, hormone therapy, or collaborative care may be appropriate.
APA citation:
Maki, P. M., Kornstein, S. G., Joffe, H., Bromberger, J. T., Freeman, E. W., Athappilly, G., Bobo, W. V., Rubin, L. H., Koleva, H. K., Cohen, L. S., & Soares, C. N. (2019). Guidelines for the evaluation and treatment of perimenopausal depression: Summary and recommendations. Journal of Women’s Health, 28(2), 117–134. https://doi.org/10.1089/jwh.2018.27099.mensocrec
2. The MENO-D: A menopause-specific depression rating scale
🩺 Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC6023883/
Summary:
This study describes the development and validation of the MENO-D, a 12-item self-report or clinician-rated scale designed to assess symptoms of perimenopausal depression. It is useful because standard depression tools may not fully capture the mood, cognitive, sleep, somatic, and hormonal-pattern symptoms that can emerge during the menopause transition.
APA citation:
Kulkarni, J., Gavrilidis, E., Hudaib, A. R., Bleeker, C., Worsley, R., Gurvich, C., & Gilbert, H. (2018). Development and validation of a new rating scale for perimenopausal depression—the Meno-D. Translational Psychiatry, 8, Article 123. https://doi.org/10.1038/s41398-018-0172-0
3. Menopause depression: Under-recognised and poorly treated
🩺 Link: https://pubmed.ncbi.nlm.nih.gov/38761367/
Summary:
This article highlights that menopause-related mental health symptoms are often missed, minimized, or treated without adequate attention to the hormonal transition itself. It discusses mood, anxiety, cognition, sleep, and neurobiological mechanisms, including the role of gonadal hormones and neurosteroids in brain function.
APA citation:
Kulkarni, J., Gurvich, C., Mu, E., & Gilbert, H. (2024). Menopause depression: Under recognised and poorly treated. Australian & New Zealand Journal of Psychiatry, 58(7), 573–575. https://doi.org/10.1177/00048674241253944
4. Sex hormones, neurotransmitters, and the adult female brain
🩺 Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC4335177/
Summary:
This review explains how ovarian hormones influence neurotransmitter systems, neural plasticity, brain structure, and functional connectivity across hormonal transition periods. It provides scientific support for understanding menopause as a brain-relevant biological transition, not simply a reproductive milestone.
APA citation:
Barth, C., Villringer, A., & Sacher, J. (2015). Sex hormones affect neurotransmitters and shape the adult female brain during hormonal transition periods. Frontiers in Neuroscience, 9, Article 37. https://doi.org/10.3389/fnins.2015.00037
5. The 2022 Hormone Therapy Position Statement of The North American Menopause Society
🩺 Link: https://pubmed.ncbi.nlm.nih.gov/35797481/
Summary:
This position statement reviews the benefits and risks of menopausal hormone therapy. It states that hormone therapy remains the most effective treatment for vasomotor symptoms and genitourinary syndrome of menopause, while emphasizing individualized care based on age, timing, health history, route, dose, duration, and use of progestogen.
APA citation:
The North American Menopause Society. (2022). The 2022 hormone therapy position statement of The North American Menopause Society. Menopause, 29(7), 767–794. https://doi.org/10.1097/GME.0000000000002028
6. The 2023 Non Hormone Therapy Position Statement of The Menopause Society
🩺 Link: https://pubmed.ncbi.nlm.nih.gov/37252752/
Summary:
This position statement reviews evidence-based nonhormonal treatments for vasomotor symptoms. It is useful for women who cannot use hormone therapy, choose not to use hormone therapy, or need additional treatment options. It includes discussion of SSRIs/SNRIs, gabapentin, fezolinetant, cognitive behavioral therapy, and other nonhormonal approaches.
APA citation:
The North American Menopause Society. (2023). The 2023 non hormone therapy position statement of The North American Menopause Society. Menopause, 30(6), 573–590. https://doi.org/10.1097/GME.0000000000002200
7. Risk for new onset of depression during the menopausal transition
🩺 Link: https://pubmed.ncbi.nlm.nih.gov/16585467/
Summary:
This study, known as the Harvard Study of Moods and Cycles, found that the menopausal transition is associated with increased risk for new-onset depressive symptoms, especially in the presence of vasomotor symptoms. It is one of the foundational studies supporting perimenopause as a window of mood vulnerability.
APA citation:
Cohen, L. S., Soares, C. N., Vitonis, A. F., Otto, M. W., & Harlow, B. L. (2006). Risk for new onset of depression during the menopausal transition: The Harvard Study of Moods and Cycles. Archives of General Psychiatry, 63(4), 385–390. https://doi.org/10.1001/archpsyc.63.4.385
8. Mood and menopause: Findings from the Study of Women’s Health Across the Nation
🩺 Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC3197240/
Summary:
This review summarizes findings from SWAN, a major longitudinal study of midlife women. It supports the finding that risk for high depressive symptoms and depressive disorder may increase during and after the menopausal transition, while also emphasizing that risk is shaped by multiple factors including prior depression, vasomotor symptoms, sleep, stress, and life context.
APA citation:
Bromberger, J. T., & Kravitz, H. M. (2011). Mood and menopause: Findings from the Study of Women’s Health Across the Nation over 10 years. Obstetrics and Gynecology Clinics of North America, 38(3), 609–625. https://doi.org/10.1016/j.ogc.2011.05.011
9. Depression in the menopause transition: Risks in the changing hormone milieu
🩺 Link: https://pmc.ncbi.nlm.nih.gov/articles/PMC6214217/
Summary:
This review discusses depression risk during the menopause transition, including the relationship between changing reproductive hormones, vasomotor symptoms, sleep disruption, prior depression history, and psychosocial stress. It is helpful for understanding why midlife mood symptoms often require a more nuanced assessment than standard depression screening alone.
APA citation:
Freeman, E. W. (2015). Depression in the menopause transition: Risks in the changing hormone milieu. Women’s Midlife Health, 1, Article 2. https://doi.org/10.1186/s40695-015-0002-y